
IMU sensors for joint kinematics
- Guest Blogger

- Mar 7, 2019
- 3 min read
Author: Elizabeth O'Keefe

The role of inertial measurement units (IMU’s) in biomechanics and orthopaedic medicine is a growing and exciting field. Kinematic analysis of joints can form an integral part of patient recovery and rehabilitation, but is currently limited by methods that are either expensive, impractical or unreliable. Optical motion capture to obtain 3D joint angles is expensive and impractical in a clinic-based setting, while “eyeballing” patient improvements and range of motions is not a reliable method for tracking patient recovery. Other clinical tools, such as goniometers, are used to measure joint angles but are limited by one dimensional measurements and do not provide an accurate or consistent positioning at a joint center.
The ability to use IMU sensors in a clinical setting to obtain 3D joint kinematics, allows for a relatively inexpensive and realistic method of measuring and quantifying patient progress and outcomes.
IMUs utilise gyroscopes, accelerometers and magnetometers to derive an object’s acceleration, angular rate and orientation relative to a global reference frame. In the past, IMUs have been used for navigation, however, the integration of IMUs and attitude and heading reference systems (AHRS) in biomechanics has allowed for a portable and wearable technique to capture body motion data (“A history of motion capture - Xsens 3D motion tracking”). Research has shown that IMUs can be calibrated for measuring knee joint rotations and are a rising tool for biomechanics and measurements of complex joints (Favre, Aissaoui, Jolles, de Guise, & Aminian, 2009).
Over the last few months EBM Analytics have been using the MTw Awinda Development Kit (Xsens Technologies B.V., Netherlands), to synthesise knee kinematics for gait analysis. This project involved the recording of gait measurements using Xsens MTws to derive meaningful data of the knee during gait. Click here to view a snippet of the sensors in action, with data being collected in real-time.
The graph below shows a sample output of the sensor data. Three Xsens MTws were adhered to the shank foot and thigh using velcro body straps, providing a non-invasive measurement method that did not obstruct knee or leg movement. The subject’s gait cycles were then normalised and compared against themselves and others. Outputs of flexion/extension (blue line), abduction/adduction (green line) and internal/external rotation angles (red line) from the recorded gait were calculated and obtained through inverse kinematics.
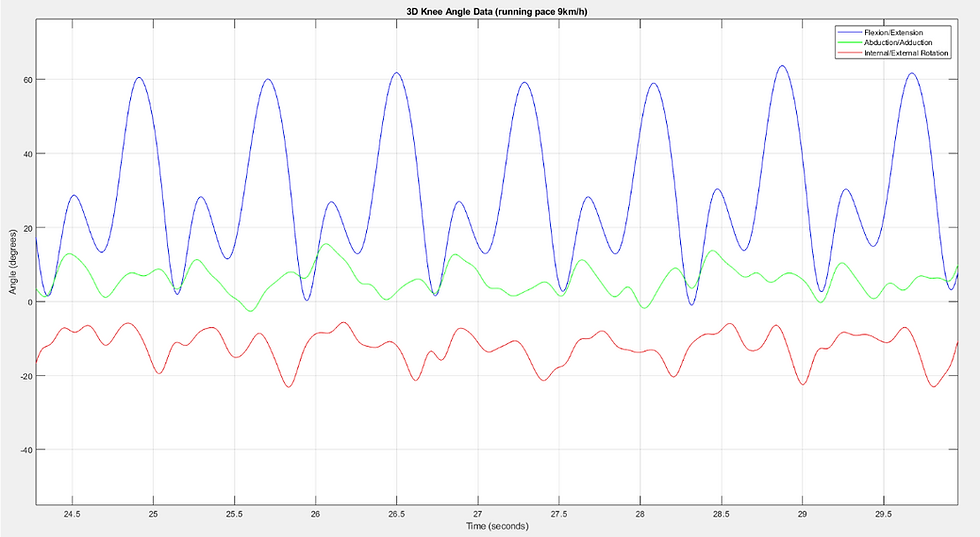
The flexion/extension angles were validated against optical motion capture using Kinovea software, giving a root mean square error (RMSE) of 1.85 between the median strides of a 3 km/h data set. This RMSE is suspected to be due to kinematic cross-talk occurring between planes, where one rotation component is interpreted as another (e.g. flexion as abduction) (Van Sint Jana, n.d.). While this system needs further validation and development, particularly for use in a clinical setting, the ability to analyse joint kinematics in an interpretable and convenient way has significant implications for quantifying patient progress and outcomes in orthopaedics and sports medicine.
References
A history of motion capture - Xsens 3D motion tracking. (n.d.). Retrieved February 20, 2019, from https://www.xsens.com/fascination-motion-capture/
Favre, J., Aissaoui, R., Jolles, B. M., de Guise, J. A., & Aminian, K. (2009). Functional calibration procedure for 3D knee joint angle description using inertial sensors. Journal of Biomechanics, 42(14), 2330–2335.
Van Sint Jana, P. S. S. S. V. S. V. F. M. R. A. S. (n.d.). Knee kinematics, Validation of a re-orientation technique of knee axis. Retrieved February 15, 2019, from https://pdfs.semanticscholar.org/c50a/cfc03534815357c4a6cab5e19029b5d3d9c5.pdf



Comments